
Recommendations of Dr Jean-Jacques Simon, Vascular Surgeon
The subclavian vein puncture, area of the axillary-subclavian junction, is known for its possible complications such as pinch-off syndrome and pneumothorax. These are perfectly avoidable when the puncture is performed under ultrasound monitoring.
Although the internal jugular vein is considered as a safe choice for a CICC (centrally inserted central catheter) or an implantable port placement, the axillary subclavian access can also be considered as a safe route. For this to be applied, there are two conditions that should be taken into consideration: the first one is to be skilled in performing central veins venipunctures, and the second one is to use real time ultrasound guidance as a systematic approach to insertion of central vascular access devices (CVADs), as stated in national and international professional recommendations (eg: SFAR – French Society of Anesthesiology and Reanimation and INS – Infusion Nurse Society). (1) (2)
The importance of ultrasound guidance in an axillary-suclavian access
 Photo 1 – Ultrasound, link between the subclavian vein, the artery and pleura – Dr Jean-Jacques Simon
Photo 1 – Ultrasound, link between the subclavian vein, the artery and pleura – Dr Jean-Jacques Simon
In fact, according to the old saying “see what you puncture and puncture what you see“, puncture under ultrasound guidance is paramount. It indeed allows a good evaluation of the vein (size, shape, depth, flow and patency). It also allows the visualization of surrounding structures to avoid (arteries, nerves, underlying pleura). Therefore, the risks related to this venous approach such as pneumothorax are avoided. Moreover, the echo-guided venipuncture takes part in the pinch-off syndrome prevention as it allows to perform puncture far from the costo-clavicular clamp area.
How to avoid pinch-off syndrome
 Photo 2 – The mechanisms of pinch-off syndrome
Photo 2 – The mechanisms of pinch-off syndrome
The “old-fashioned” puncture (catheter A) in the costo-clavicular clamp is still often used and should be abandoned. In fact, with this technique, the catheter passes through the clamp before reaching the vein. The incessant “jaw” movements of the clamp will crush the catheter between the clavicle, the first rib, and the scythe of the subclavian muscle. This creates a high risk of rupture and migration of the catheter towards the right cavities or even the pulmonary artery.
Puncture under ultrasound (catheter B) mitigates the risk because the catheter passes “offshore”.
With a catheter already implanted in the arm and therefore, inserted higher up in the vein, the risk can also be avoided. This is the case when using a PICC-line for instance (catheter C).
In practice, having to position the arm in abduction to facilitate injection implies that the catheter is pinched, which is an indicator of pinch-off syndrome stage I.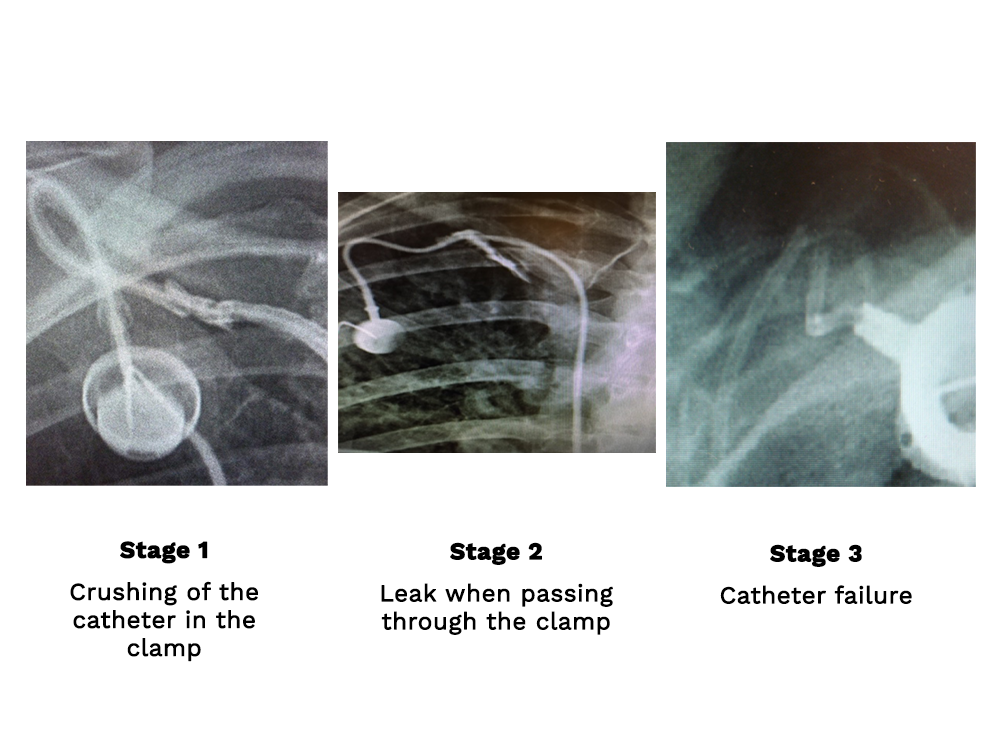 Photo 3 – The three stages of pinch-off – Dr Jean-Jacques Simon
Photo 3 – The three stages of pinch-off – Dr Jean-Jacques Simon
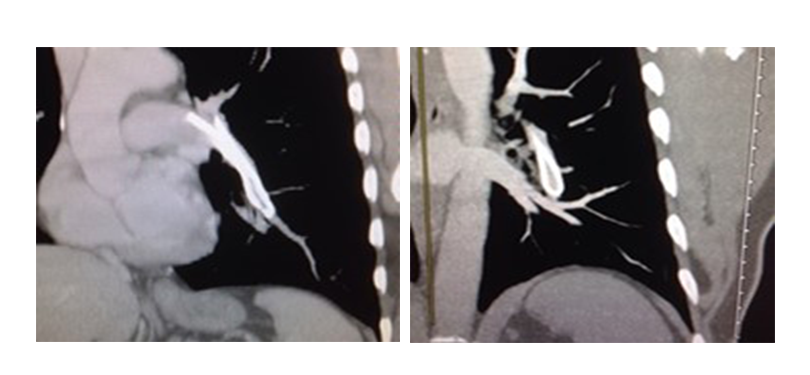 Photo 4 – Catheter embolization in pulmonary artery, consequence of stage 3 of pinch-off – Dr Jean-Jacques Simon
Photo 4 – Catheter embolization in pulmonary artery, consequence of stage 3 of pinch-off – Dr Jean-Jacques Simon
The axillary-subclavian access: between safety and aesthetics
The axillo-subclavian access is not only safe, but it has also the great advantage of being aesthetic.
The catheter is not visible under the skin when it is in front of the clavicle and in its path between the jugular vein and the implantable port.
A single incision approach in an axillary fold is also possible. The vein is then punctured from the incision using ultrasound guidance.
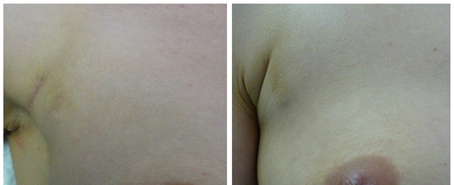 Photo 5 – Hidden scars – Dr Jean-Jacques-Simon
Photo 5 – Hidden scars – Dr Jean-Jacques-Simon
Conclusion
As stated earlier, I recommend using the axillary-subclavian access only if one is experienced in ultrasound guidance and has good prior experience in jugular puncture.
It is important to abstain from using it if the vein is small, deep, in an overweight patient, in the presence of contralateral thoracic pathology and especially if a contralateral pneumonectomy has been performed.
Until now, the axillary-subclavian access was mainly considered as an alternative in the case case of an unusable internal jugular vein. However, if all the recommendations described in this article are gathered, it no longer deserves its reputation and can be approached in primary intention.
Bibliography
- French Society of Anesthesiology and Reanimation (SFAR) – Recommandations sur l’utilisation de l’échographie lors de la mise en place des accès vasculaires – https://sfar.org
- INS Standards of Practice 2021 – https://www.ins1.org/publications/infusion-therapy-standards-of-practice/
- Schulman PM, Gerstein NS, Merkel MJ, Braner DA, Tegtmeyer K, Ultrasound-guided cannulation of the subclavian vein, N Engl J Med 2018; 379:e1
- JJ Simon – Chambre implantable : un jeu de massacre, DIVLD Congress 2014
If you liked this article, you may also like:




0 Comments
Trackbacks/Pingbacks