
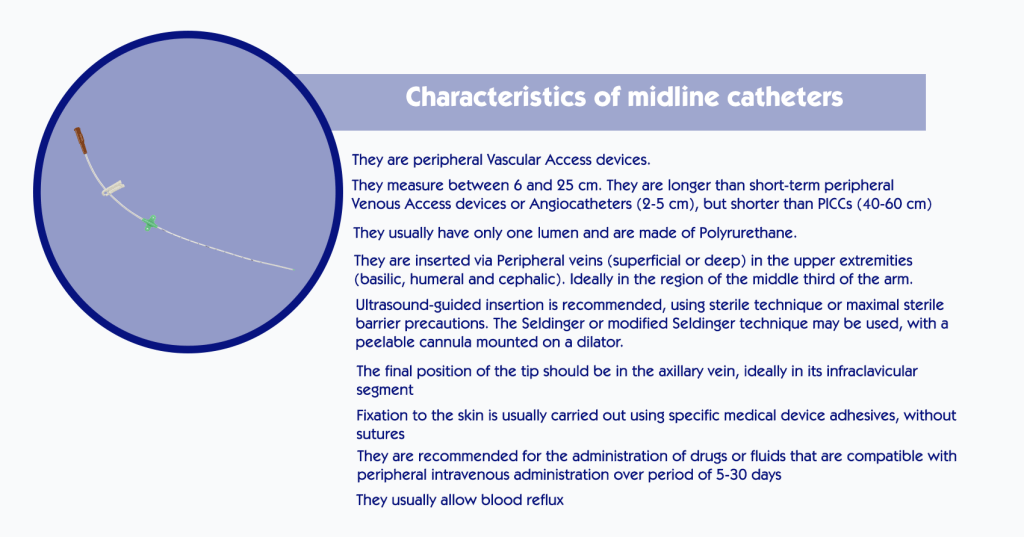
The characteristics that define midline catheters are well established. However, in recent years a new group of peripheral vascular access devices has appeared on the market: long peripheral catheters (long peripheral IV catheters), also known as “mini-midlines”. The characteristics of both devices are summarised in Figures 1 and 2.

As shown in Figure 3, catheters that are inserted via a vein in the arm (superficial or deep) and whose tip is located in the axillary vein (ideally in its infraclavicular segment) should, strictly speaking, be regarded as midline catheters.

Any other catheter inserted into the veins of the extremities should be referred to as a peripheral venous catheter, either short (if less than 5 cm) or long (if 6 cm or more, and its tip does not progress beyond the root of the limb).
Peripherally inserted catheters whose tip is located in central veins of the upper region (subclavian, brachiocephalic or superior vena cava), of the lower region (femoral, iliac or inferior vena cava) or in the right atrium, should be referred to as peripherally inserted central catheters (PICCs).
II. Indications and contraindications
Various good clinical practice guidelines, both for adult and paediatric patients (Figure 4), as well as medical associations related to vascular access care, recommend the use of midline catheters in the following situations:
– Administration of intravenous treatments of intermediate duration (between 5-7 days and 1 month), provided that they are compatible with peripheral intravenous administration.
– Need for frequent blood draws. Since the axillary vein is usually of considerable calibre, midline catheters very often allow blood to be drawn through it.
– Patients with reduced peripheral venous integrity, regardless of the duration of treatment. Ultrasound-guided insertion into veins in the arm reduces exhaustion of the veins associated with multiple venipunctures, particularly in chronic or complex patients.

Despite these recommendations, the fact is that in current clinical practice midline catheters are still rarely used in children. The persistent lack of training in vascular access care and in the use of ultrasound, as well as the limited market availability of small-calibre midline catheters appropriate for use in children, could provide at least a partial explanation for this reality.
The contraindications for midline catheters are:
– Need to administer drugs or fluids not compatible with peripheral infusion. Vesicant, irritant or centrally administered drugs or fluids (pH > 9, pH < 5, osmolarity > 600 mOsm/L) should be administered by peripherally inserted central venous catheters (PICCs), non-tunnelled centrally inserted catheters (CICCs) or tunnelled centrally inserted catheters (Hickman™ or Port-A-Cath™ type).
– Absence of peripheral veins of sufficient calibre. With the aim of preserving peripheral venous integrity and avoiding complications in the form of phlebitis and thrombosis, it may be reasonable to avoid the use of these catheters in children with very small calibre veins (< 2 mm). To determine whether the child is a good candidate for midline catheter placement, and to optimise the selection of the vein to be cannulated and the calibre of the catheter to be inserted, it is therefore highly advisable to first assess vascular integrity using ultrasound. Placement of 2, 3 or 4 Fr midline catheters should thus be considered for children with veins larger than 2, 3 or 4 mm in diameter, respectively.
– Patients in whom sedation or anaesthesia for catheter insertion is contraindicated.
III. Clinical applications in paediatric patients

The stability offered by these catheters, although probably inferior to that of PICCs, could make it possible to manage a significant percentage of children on an outpatient basis. This is extremely important for paediatric patients, not only because it can significantly reduce care costs, but also because it increases the child’s well-being, enables family life and reduces school absenteeism.
Venipuncture causes anxiety and pain, and can destabilise children with respiratory or haemodynamic dysfunction. Midline catheters can therefore play a key role in avoiding unnecessary suffering in the child, minimising the exhaustion of peripheral venous integrity by avoiding repeated punctures, and greatly facilitating the work of nursing staff.
Their use could be particularly advantageous in hospitals that treat a significant volume of children with chronic or complex diseases, where multiple blood draws are often required during hospitalisation.
Traditionally, it was recommended that polyurethane catheters, 3 French or larger, were inserted if reflux was necessary, which could limit their insertion in infants or young children.
Such a wide range of lengths and gauges makes them tremendously versatile and they can be used in children and adults as long peripheral cannulas, as a midline catheter or even as PICCs in young children.
The catheter tip is curved or tapered, and is inserted by means of the Seldinger technique, without using peelable sheath, thus minimising vessel wall trauma and facilitating ultrasound-guided insertion.
In addition, they are made of highly resistant polyurethane. This, in turn, offers two advantages.
Firstly, these catheters can withstand high pressure injections (between 150 psi, the 2 French, and 300 psi, the 5 French) and allow the administration of fluids at high flow rates (between 1.5 mL/s, the 2 French, and 5 mL/s, the 4 French). This could lead to their use for the stabilisation and subsequent management of severely ill children who are haemodynamically unstable, who require rapid administration of fluids or blood products, or who need to be administered intravenous contrast for imaging tests. However, in this type of patient the peripheral venous system often collapses, making it difficult or impossible to insert peripheral catheters even with ultrasound guidance. In these cases, and in those in which an emergency infusion of catecholamines is indicated, the insertion of a CICC will be indicated.
Secondly, as they are made of highly resistant polyurethane, they have a larger internal section, facilitating the reflux of blood into the catheter.
Conclusion
Good clinical practice guidelines recommend the use of midline catheters in children who require intravenous treatments lasting more than five days, provided the drugs or fluids are compatible with peripheral venous administration.
They can also be useful in children who require frequent blood draws, especially if they are chronically ill or complex, where it is essential to preserve peripheral venous integrity. The recent commercialisation of high-flow, small-calibre mid-line catheters broadens the scope for their use in paediatric patients.
Bibliography
• Adams DZ, Little A, Vinsant C, Khandelwal S. The Midline Catheter: A Clinical Review. J Emerg Med. 2016;51(3):252-8.
• Cotogni P and Pittirutti M. Focus on peripherally inserted central catheters in critically ill patients. World J Crit Care Med 2014; 3(4): 80-94.
• Pacilli M, Bradshaw CJ, Clarke SA. Use of 8-cm 22G-long peripheral cannulas in pediatric patients. J Vasc Access. 2018;19(5):496-500.
• Anderson J, Greenwell A, Louderback J, Polivka BJ, Behr JH. Comparison of outcomes of extended dwell/midline peripheral intravenous catheters and peripherally inserted central catheters in children. JAVA 2016;21(3):158-64.
• Qian SY, Horn MT, Barnes R, Armstrong D. The use of 8-cm 22G Seldinger catheters for intravenous access in children with cystic fibrosis. J Vasc Access 2014;15: 415-7.
• Ozkiraz S, Gokmen Z, Anuk Ince D, Akcan AB, Kilicdag H, Ozel D, Ecevit A. Peripherally inserted central venous catheters in critically ill premature neonates. J Vasc Access. 2013;14(4):320-4.
• Scott-Warren VL, Morley RB. Paediatric vascular access. BJA Education. 2015;15(4):199-206.
• Moureau N and Chopra V. Indications for peripheral, midline and central catheters: summary of the MAGIC recommendations. Br J Nurs 2016; 25(8): S15-S24.
• Scoppettuolo G, Pittiruti M, Pitoni S, Dolcetti L, Emoli A, Mitidieri A, Migliorini I, Annetta MG. Ultrasound guided ‘short’ midline catheters for difficult venous access in the emergency department: a retrospective analysis. Int J Emerg Med 2016;9(1):3.
• Griffiths V. Midline catheters: indications, complications and maintenance. Nurs Stand. 2007;22(11):48-57.
• Alexandrou E, Ramjan LM, Spencer T, Frost SA, Salamonson Y, Davidson PM, Hillman KM. The use of midline catheters in the adult acute care setting: clinical implications and recommendations for practice. J Assoc Vasc Access. 2011;16(1):35-41.
• Cummings M, Hearse N, McCutcheon H, Deuter K. Improving antibiotic treatment outcomes through the implementation of a midline: piloting a change in practice for cystic fibrosis patients. J Vasc Nurs. 2011;29(1):11-15.
• Caparas JV, Hu J-P. Safe administration of vancomycin through a novel midline catheter: a randomized, prospective clinical trial. J Vasc Access. 2014;15(4):251-256.
• Moureau N, Sigl G, Hill M. How to establish an effective midline program: a case study of 2 hospitals. J Assoc Vasc Access. 2015;20(3):179-188.




0 Comments
Trackbacks/Pingbacks