
In modern healthcare, multiple professionals are responsible of inserting vascular access devices in patients. Within the same hospital, different categories of professionals end up using the same type of catheters. However, when each of these professionals employs their own insertion technique, it hinders the establishment of an objective and measurable system that would enhance error prevention and minimize complications.
In response to the advancements in medical practices over recent decades, standardization has become common in the healthcare industry. This approach ensures predictable and measurable outcomes. Furthermore, the adoption of systematic methods streamlines the process of teaching and learning, leading to a more consistent execution of procedures.
Therefore, it harmonizes the actions of a group of individuals, all working towards the same goal: in this case, healthcare professionals striving for the most appropriate solution to address the health issues of the population. In this article, we present an in-depth overview of the SIP-2 protocol, an effective technique for the insertion of PICC catheters.
What is the SIP-2 protocol?
The SIP (Safe Insertion of PICCs) protocol was established nearly a decade ago by the GAVeCeLT group to disseminate a standardized and evidence-based approach for PICC (Peripherally Inserted Central Catheter) insertion. As medical practices have rapidly evolved, a second version of the protocol has been developed that aims for accurate PICC placement all while minimizing complications.
How does the SIP-2 protocol work?
The SIP-2 protocol consists of 8 steps, as originally presented in 2014, but it has undergone updates over time, which are also included in this piece:
> HAND WASHING, STERILE TECHNIQUE, 2% ALCOHOLIC CHLORHEXIDINE DISINFECTION:
The PICC insertion technique is a sterile procedure, and as such, it requires maximum barrier measures, including:
- Surgical handwashing
- Use of a cap, mask, sterile gloves, and sterile gown
- A large sterile drape covering the patient
- Use of a long cover for the ultrasound probe.
While a dedicated room is not essential for PICC insertion, as it can be performed at the bedside, it is advisable to create a comfortable environment for the patient, promoting a faster and more pleasant insertion experience for both them and the healthcare professional.
The skin disinfection should be carried out using 2% alcoholic chlorhexidine with vigorous friction for at least 30 seconds before placing the sterile sheet.
 Image 1: A nurse performing PICC insertion. Sterile gloves, sterile gown, cap, mask, cover for the ultrasound probe, and a large sterile drape with a fenestration for the arm area are visible as part of the SIP-2 protocol. Source: Gloria Ortiz.
Image 1: A nurse performing PICC insertion. Sterile gloves, sterile gown, cap, mask, cover for the ultrasound probe, and a large sterile drape with a fenestration for the arm area are visible as part of the SIP-2 protocol. Source: Gloria Ortiz.
> EXPLORATION OF ALL ARM AND NECK VEINS – RAPEVA
The use of an ultrasound machine allows us to assess the patient’s venous system before puncturing for the procedure. We use a systematic method of ultrasound scanning called RaPeVA, which stands for Rapid Peripheral Vascular Assessment. This allows us to observe the deep vascular structures of the patient and understand the unique aspects of their anatomy.
 Image 2: Dr. Pittiruti performing RaPeVA on a healthy volunteer during a practical workshop for nurses. Source: Gloria Ortiz.
Image 2: Dr. Pittiruti performing RaPeVA on a healthy volunteer during a practical workshop for nurses. Source: Gloria Ortiz.
This method provides us with the necessary information to proceed with the procedure safely. In practice, it is common to see it associated with the RaCeVA method (Rapid Central Vascular Assessment), which is a rapid assessment of central veins.
> CHOOSING THE MOST APPROPRIATE VEIN:
Thanks to RaPeVA, we can select the most suitable vein for catheter insertion based on these parameters:
- Depth: It is generally not recommended to puncture PICCs if the vein is more than 3cm deep.
- Proximity of the vein to other structures that should not be damaged, such as nerves and arteries.
- Ability to collapse under pressure applied by the ultrasound probe, indicating that the vein is patent.
- Diameter: Essential information when choosing the catheter size, which should not exceed one-third of the vein’s size to avoid complications like thrombosis (image 3).
On the other hand, the preferred vein should be located in the green zone of Dawson, which is the ideal area for puncture and catheter fixation. If the vein is in the yellow zone of Dawson, tunnelling to the green zone should be performed, as it is cleaner and more stable.
 Image 3: Ultrasound image of a vein with a diameter of 0.43cm (indicated in the lower-left corner of the image). Source: Maite Parejo.
Image 3: Ultrasound image of a vein with a diameter of 0.43cm (indicated in the lower-left corner of the image). Source: Maite Parejo.

> IDENTIFICATION OF THE MEDIAN NERVE AND BRACHIAL ARTERY:
During RaPeVA, in addition to choosing the vein for puncture, special attention must be given to visualizing and identifying structures that should not be damaged, such as the brachial artery and median nerve.
Both structures are found in the brachial bundle, commonly referred to as the “Mickey Mouse head”. The artery has a distinctive circular shape, a pulsating rhythm and remains visibile under pressure from the ultrasound probe. It resembles the “head” of Mickey Mouse.
 Image 4 A: Brachial artery marked in the red circle, located within the brachial bundle. Source: Maite Parejo.
Image 4 A: Brachial artery marked in the red circle, located within the brachial bundle. Source: Maite Parejo.

The nerve can be more challenging to identify: the literature describes it as a structure with a “honeycomb” appearance that resists to pressure and can be positioned differently around the brachial bundle.
 Image 4 B: Median nerve marked in the yellow circle, located within the brachial bundle. Source: Maite Parejo.
Image 4 B: Median nerve marked in the yellow circle, located within the brachial bundle. Source: Maite Parejo.

> USE OF ULTRASOUND FOR PUNCTURE + MODIFIED SELDINGER TECHNIQUE (IMAGE 5 A AND B):
Ultrasound increases the success rate of vein puncture on the first attempt and allows for precise control of the needle during insertion.
International guidelines recommend using ultrasound for vascular puncture due to its safety and cost-effectiveness. Additionally, the use of the modified Seldinger technique (which includes a 21G echogenic needle, nitinol wire with a soft tip, and peelable microintroducer) enables work on small-caliber vessels in the arm, reducing potential endothelial damage from venous puncture and catheter insertion.
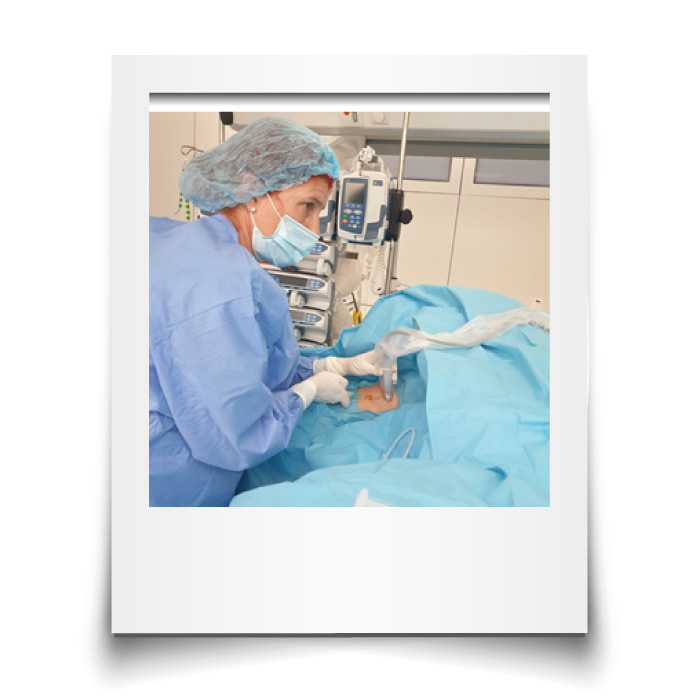 Image 5 A: Nurse performing ultrasound-guided anesthesia before PICC insertion. Source: Gloria Ortiz.
Image 5 A: Nurse performing ultrasound-guided anesthesia before PICC insertion. Source: Gloria Ortiz.
 Image 5 B: Nurse advancing the soft-tip nitinol wire through a 21G micropuncture needle. Source: Gloria Ortiz.
Image 5 B: Nurse advancing the soft-tip nitinol wire through a 21G micropuncture needle. Source: Gloria Ortiz.
> ULTRASOUND MONITORING OF THE INTERNAL JUGULAR VEIN DURING CATHETER PROGRESSION:
During PICC insertion, it is beneficial to visualize the internal jugular vein on the same side of the insertion using ultrasound. Slightly compressing the vein with the ultrasound probe helps facilitate the passage of the catheter through the subclavian vein into the brachiocephalic vein without shifting towards the internal jugular vein.
 Image 6: The orange arrow indicates the previously positioned internal jugular vein anterior to the carotid artery. Source: Maite Parejo.
Image 6: The orange arrow indicates the previously positioned internal jugular vein anterior to the carotid artery. Source: Maite Parejo.

> USE OF INTRACAVITARY ECG FOR TIP VERIFICATION:
As soon as the catheter tip reaches the lower region of the superior vena cava, the intracavitary P wave will start to increase in size, indicating the correct tip position at its maximum amplitude without a negative wave. The “column of saline” technique is commonly employed during PICC insertion to achieve this positioning.

Image 7: The screen displays the top line corresponding to the surface ECG and the bottom line showing the intracavitary ECG with a clear, non-biphasic intracavitary P wave, indicating the correct positioning of the catheter tip at the cavo-atrial junction.
> USE OF SUTURELESS FIXATION SYSTEM + CYANOACRYLATE + TRANSPARENT MEMBRANE:
International guidelines strongly discourage using sutures to secure vascular catheters. Evidence shows that sutures increase the risk of accidental needlestick injuries on healthcare professionals, the risk of thrombosis and infection, and can cause discomfort for the patient, particularly in certain anatomical areas.
Sutureless fixation systems can be adhesive or subcutaneous. The latter is recommended for patients who need the catheter to remain in place for more than 3 weeks, have delicate skin or MARSI (Medical Adhesive-Related Skin Injuries), are at risk of accidental dislodgment, or in non-cooperative patients (e.g., disoriented, children, neonates) (Image 8).
 Image 8: PICC catheter secured with a subcutaneous anchor. Source: Maite Parejo.
Image 8: PICC catheter secured with a subcutaneous anchor. Source: Maite Parejo.
The use of cyanoacrylate at the insertion site helps achieve hemostasis and controls any potential post-insertion bleeding. It allows for the first dressing change to be done after one week, instead of within the first 24 hours. Additionally, cyanoacrylate acts as a sterile protective barrier over the insertion site while it is in place.
The transparent semipermeable membrane provides direct observation of the insertion site and effective covers the surrounding skin. It is recommended to select membranes with high breathability to prevent moisture buildup under the dressing, which could lead to skin maceration.
Dr. Pittiruti and his team have announced that a new version of the SIP-2 protocol will be published soon. We can expect to see some updates based on the latest evidence.
Familiarizing oneself with PICC insertion, especially with ultrasound guidance, involves a significant learning curve. Adopting a protocol like the SIP-2 protocol can greatly enhance the teaching and learning process for this technique. The clear and simple steps outlined by the GAVeCeLT group in this proposal can enable vascular access professionals to approach these practices with ease and make faster progress.
BIBLIOGRAPHY:
Infusion Nursing Society Guidelines, 2021.
Emoli A, Cappuccio S, Marche B, Musarò A, Scoppettuolo G, Pittiruti M; Gruppo Aperto di Studio sugli Accessi Venosi Centrali a Lungo Termine. Il protocollo ‘ISP’ (Inserzione Sicura dei PICC): un “bundle” di otto raccomandazioni per minimizzare le complicanze legate all’impianto dei cateteri centrali ad inserimento periferico (PICC). Assist Inferm Ric. 2014 Apr-Jun;33(2):82-9. Italian. doi: 10.1702/1539.16813. PMID: 25002059.
Spencer TR, Pittiruti M. Rapid Central Vein Assessment (RaCeVA): A systematic, standardized approach for ultrasound assessment before central venous catheterization. J Vasc Access. 2019 May;20(3):239-249. doi: 10.1177/1129729818804718. Epub 2018 Oct 4. PMID: 30286688.
Ostroff MD, Moureau N, Pittiruti M. Rapid Assessment of Vascular Exit Site and Tunneling Options (RAVESTO): A new decision tool in the management of the complex vascular access patients. J Vasc Access. 2021 Jul 21:11297298211034306. doi: 10.1177/11297298211034306. Epub ahead of print. PMID: 34289721.
Pittiruti M, Pelagatti F, Pinelli F. Intracavitary electrocardiography for tip location during central venous catheterization: A narrative review of 70 years of clinical studies. J Vasc Access. 2021 Sep;22(5):778-785. doi: 10.1177/1129729820929835. Epub 2020 Jun 24. PMID: 32578489.
Dawson, R. PICC Zone Insertion Method™ (ZIM™): A systematic approach to determine the ideal insertion site for PICCs in the upper arm. JAVA. 2011. 16(3): 156-165. DOI: 10.2309/java.16-3-5




0 Comments